
Introduction
- Delta wave is a typical ECG pattern for preexcitation of ventricular myocardium
- Preexcitation occurs when impulses from atrium are conducted via an accessory pathway (AP) that directly connects the atria and ventricles and bypasses the AV node This results in the earlier activation of the ventricles than if the impulse had travelled through the AV node
- Accessory pathways or bypass pathways are strands of myocardium that are created by incomplete embryological development of the AV annuli. They may be located anywhere along the AV ring or in the septum, but most commonly found along mitral or tricuspid annulus
- These pathways may conduct antegrade only, retrograde only, or antegrade and retrograde. Retrograde only pathways cannot be seen on the ECG
- Various algorithms can help determine pathway location, but the same pathway may not always produce the identical ECG pattern. Furthermore 13% of patients with preexcitation have more than one accessory pathway
Classification
Types of accessory pathways:
- bundle of Kent – classical type of AV bypass tract in WPW pattern
- James fibers - atrio-nodal tracts, these connect atrium to distal or compact AV node
- Brechenmacher fibers (atrio-Hisian tracts) - connecting the atrium to His bundle
- Mahaim fibers - Hisian-fascicular tracts connect the atrium (atriofascicular pathways), AV node (nodofascicular pathways) or His bundle (fasciculoventricular) to distal Purkinje fibers or ventricular myocardium
Clinical manifestations
Wolff Parkinson White syndrome
- pre-excitation caused by accessory pathway - usually the Kent bundle, which directly links the atria to the ventricles, bypassing the atrioventricular (AV) node in combination with recurrent atrioventricular reentrant tachycardia
- The prevalence of WPW pattern is estimated at 0.13 to 0.25 % in the general population
- WPW can be divided by position of accessory pathway to:
- Type A - left sided accessory pathway resulting in tall R wave in leads V1-V3 (a positive or upward delta wave)
- Type B - right sided accessory pathway in which there are QS complexes in leads V1-V3 (a negative or downward delta wave)
The majority of patients with the WPW pattern on their ECG remain asymptomatic, although a small percentage of patients with the WPW pattern develop arrhythmias as a part of WPW syndrome.
The most frequent WPW associated tachycardia is AVRT.
Atrioventricular reentrant tachycardia (AVRT)
- AVRT is a supraventricular tachycardia that utilizes an accessory pathway between the atria and ventricles resulting in a circus movement.
- It is frequently, but not exclusively, associated with preexcitation syndrome (ie, the Wolff-Parkinson-White syndrome).
- The circuit involved in this reentrant arrhythmia includes the accessory bypass tract, AV node, and His Purkinje system, as well as the atria and ventricles.
- There is always 1:1 conduction of the impulse between the atria and ventricles since both structures, along with the AV node and accessory pathway, are a necessary part of the circuit.
- AVRT is often triggered by premature atrial beats or premature ventricular beats – retrograde activation of atria.
- Orthodromic AVRT accounts for >90% of AVRT and 20-30% of all sustained SVT.
Orthodromic AVRT
- >90% of AVRT
- re-entrant impulse goes from the atrium to the ventricle through the AV node (normal ventricular activation) and then retrogradely activates atria through accessory pathway
- ECG:
- narrow complex tachycardia
- ventricular rate 150-250 bpm
- inverted P wave following a QRS complex - retrograde activation of the atrium
- short RP interval that is usually less than half of RR interval (< ½ RR)
Antidromic AVRT
- the least common arrhythmia associated with WPW syndrome (3-8% of patients)
- Ventricles are activated through a very fast-conducting accessory pathway – anterograde conduction, atria are retrogradely activated over the AV node or another accessory pathway (30-60% of patients have multiple accessory pathways).
- ECG:
- wide QRS complex tachycardia
- ventricular rate 150-250 bpm
- Inverted P waves are often hidden in ST-T segment and therefore the RP interval is usually difficult to assess
Picture 1 Visualization of accessory pathway (bundle of Kent)

http://ems12lead.com/2012/02/06/discussion-for-17-year-old-male-cc-chest-pain-and-palpitations-wpw-part-i/#gref
Lown- Ganong-Levine syndrome
- short PR interval
- The exact mechanism of LGL has not been completely described. It’s most likely due to rapidly conducting fibers within the AV node
- Conduction occurs more rapidly than normal from the atria to the ventricles, explaining the short PR. The QRS complex is normal in duration and morphology since ventricular activation is via the normal conduction pathway.
Accessory pathway as a bystander
- In the presence of focal AT, atrial flutter, AF, or AVNRT
- QRS complexes can be pre-excited with delta waves when the AP acts as a bystander, and is not a critical part of the re-entry circuit.
FBI = Fast Broad Irregular tachycardia
- this arrhythmia represents a pre-excited atrial fibrillation
- Paroxysmal AF has been found in 50% of patients with WPW
- Typically young patients with no structural disease of the heart
- atrial fibrillation with fast ventricular response over an accessory pathway
- potentially life-threatening arrhythmia – due to 1:1 conduction the ventricular rate may be very rapid (even >300bpm) and it can degenerate into ventricular fibrillation!
ECG of atrial fibrillation in WPW:
- irregular wide complex tachycardia
- ventricular rate >200 bpm
- QRS complexes usually have variable morphology – APs bypassing the AV node can produce wide and bizarre looking complexes
- axis remains stable
Permanent junctional reciprocating tachycardia (PJRT)
- PJRT is a rare form of AV reciprocating tachycardia using a concealed AP
- Accessory pathways are usually located in the posteroseptal region and are associated with retrograde conduction
- PJRT is a long RP tachycardia due to slow conduction properties of the AP
- characterized by deeply inverted retrograde P waves in leads II, III, and aVF
- The incessant nature of PJRT may result in tachycardiomyopathy (TCM) that usually resolves after successful treatment by radiofrequency catheter ablation
ECG features of preexcitation
- preexcitation has a typical pattern during sinus rhythm:
- the PR interval is short
- delta wave - the initial part of ventricular activation is slowed, and the upstroke of the QRS complex is slurred, because of slow muscle-fiber-to-muscle-fiber conduction.
- wide QRS complex >120ms - the QRS complex represents a fusion beat - the initial part results from slow ventricular activation via the accessory pathway, while the terminal portion of ventricular activation is via the normal conduction system.
- ST segment and T wave abnormalities - reflecting abnormal ventricular repolarization.
- ST-T segment is usually directed opposite to delta waves > positive delta wave is often followed with a descending ST segment and inverted T wave.
- The more rapid the conduction along the accessory pathway, the greater the amount of myocardium depolarized via the accessory pathway > resulting in a more prominent or wider delta wave, and increasing prolongation of the QRS complex.
Delta waves can be misinterpreted as a different diagnosis due to similar patterns as:
- Myocardial infarction (MI) – A negative delta wave presented as a Q wave. On the other hand, a positive delta wave may mask the presence of a previous MI
- Ventricular premature beats (VPBs) or idioventricular rhythm – Intermittent WPW may be mistaken for frequent VPBs.
- Bundle branch block – The QRS duration is equal to or greater than 0.12 seconds because of preexcitation (the delta wave). Right-sided pre-excitation can be mistaken for LBBB; left sided pre-excitation can be mistaken for RBBB
Various algorithms have been developed to help determine pathway location from surface ECG. One of those is for example St. George’s algorithm:
Picture 2

BRUGADA and col. 2019 Guidelines on Supraventricular Tachycardia (for the management of patients with) [online]. [cit. 4.2.2021]. Accessible at WWW: https://academic.oup.com/eurheartj/article/41/5/655/5556821
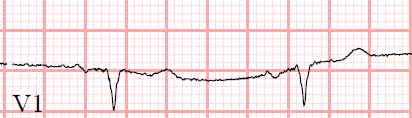
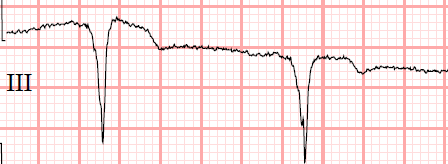
ECG 1
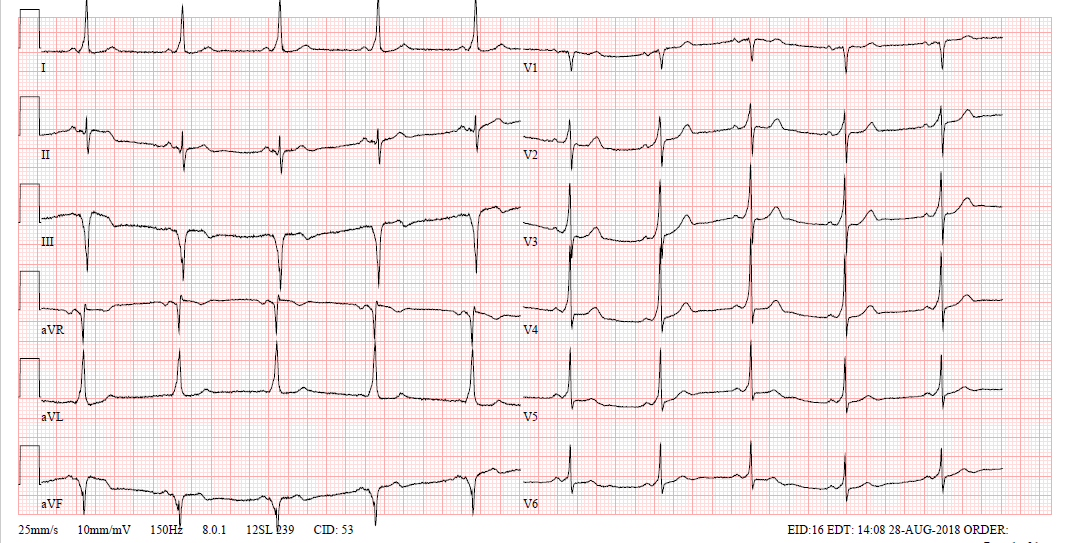
Delta waves during sinus rhythm
- sinus rhythm at a rate of 60 bpm
- PR interval is shorter around 120ms
- typical sloping delta waves in every lead
- QRS complex is wide >120ms
- using St. George’s algorithm, we can approximate localization of the accessory pathway
- negative QRS complexes in leads V1 and III
- and negative QRS in lead aVF
- from there we can see highest R in lead V4 and R
- in conclusion the accessory pathway is probably located in mid septal region

ECG 2
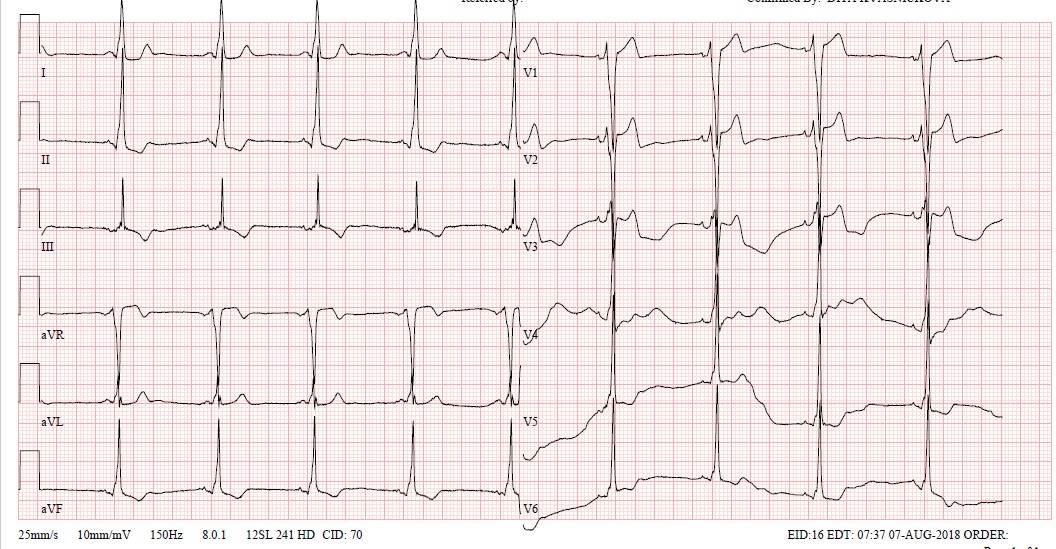
Sinus rhythm with delta waves
- sinus rhythm at a rate of 57 bpm
- short PR interval – 90ms
- delta waves present
- wide QRS complexes – 150ms
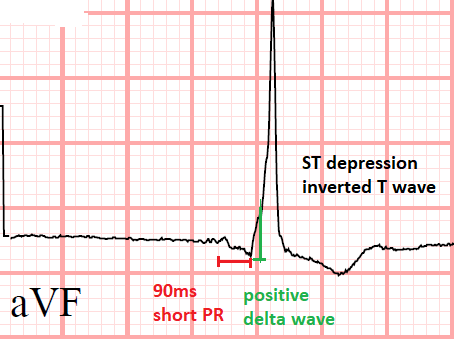
- ST segment and T waves abnormalities – in leads II, III, aVF descending ST depression and inverted T wave with preceding positive delta wave
- location of accessory pathway by St. George’s algorithm – Right lateral location
- negative QRS in V1, positive QRS in III, positive QRS in aVL
Management
- risk stratification of asymptomatic patients with WPW pattern on a surface ECG using non-invasive tests (exercise ECG) or an electrophysiologic study
- Recommended long-term treatment for symptomatic patients is catheter ablation of the accessory pathway. Precise localization of the anomalous pathway is critical for successful ablation
- Symptomatic patients with tachyarrhythmias should be treated accordingly for the specific type of pre-excited arrhythmia.
References
- CAMM, A. J., LÜSCHER, T. F., & SERRUYS, P. W. (2009). The ESC textbook of cardiovascular medicine. Oxford, Oxford University Press
- Brugada J, Katritsis DG, Arbelo E, Arribas F, Bax JJ, Blomström-Lundqvist C, Calkins H, Corrado D, Deftereos SG, Diller GP, Gomez-Doblas JJ, Gorenek B, Grace A, Ho SY, Kaski JC, Kuck KH, Lambiase PD, Sacher F, Sarquella-Brugada G, Suwalski P, Zaza A; ESC Scientific Document Group. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J. 2020 Feb 1;41(5):655-720. doi: 10.1093/eurheartj/ehz467. PMID: 31504425.
- Jordan M Prutkin, MD, MHS, FHRS (2019). ECG tutorial: Preexcitation syndromes. In I. Gordon M Saperia, MD (Ed.), UpToDate. Retrieved February 3, 2021, from https://www-uptodate-com.ezproxy.is.cuni.cz/contents/ecg-tutorial-preexcitation-syndromes?search=preexcitation%20syndrome&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2
- Bradley P Knight, MD, FACC (2019). Anatomy, pathophysiology, and localization of accessory pathways in the preexcitation syndrome. In I. Todd F Dardas, MD, MS (Ed.), UpToDate. Retrieved February 3, 2021 from https://www-uptodate-com.ezproxy.is.cuni.cz/contents/anatomy-pathophysiology-and-localization-of-accessory-pathways-in-the-preexcitation-syndrome?search=preexcitation%20syndrome&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
- Luigi Di Biase, MD, PhD, FHRS, Edward P Walsh, MD (2019). Wolff-Parkinson-White syndrome: Anatomy, epidemiology, clinical manifestations, and diagnosis. In I. Todd F Dardas, MD, MS (Ed.), UpToDate. Retrieved February 3, 2021 from https://www-uptodate-com.ezproxy.is.cuni.cz/contents/wolff-parkinson-white-syndrome-anatomy-epidemiology-clinical-manifestations-and-diagnosis?search=preexcitation%20syndrome&source=search_result&selectedTitle=3~150&usage_type=default&display_rank=3
Pictures
- BAUMRIND, David. EMS 12-Lead [online]. [cit. 3.2.2021]. Accessible at WWW: http://ems12lead.com/2012/02/06/discussion-for-17-year-old-male-cc-chest-pain-and-palpitations-wpw-part-i/#gref
- BRUGADA and col. 2019 Guidelines on Supraventricular Tachycardia (for the management of patients with) [online]. [cit. 4.2.2021]. Accessible at WWW: https://academic.oup.com/eurheartj/article/41/5/655/5556821

Introduction
- Delta wave is a typical ECG pattern for preexcitation of ventricular myocardium
- Preexcitation occurs when impulses from atrium are conducted via an accessory pathway (AP) that directly connects the atria and ventricles and bypasses the AV node This results in the earlier activation of the ventricles than if the impulse had travelled through the AV node
- Accessory pathways or bypass pathways are strands of myocardium that are created by incomplete embryological development of the AV annuli. They may be located anywhere along the AV ring or in the septum, but most commonly found along mitral or tricuspid annulus
- These pathways may conduct antegrade only, retrograde only, or antegrade and retrograde. Retrograde only pathways cannot be seen on the ECG
- Various algorithms can help determine pathway location, but the same pathway may not always produce the identical ECG pattern. Furthermore 13% of patients with preexcitation have more than one accessory pathway
Classification
Types of accessory pathways:
- bundle of Kent – classical type of AV bypass tract in WPW pattern
- James fibers - atrio-nodal tracts, these connect atrium to distal or compact AV node
- Brechenmacher fibers (atrio-Hisian tracts) - connecting the atrium to His bundle
- Mahaim fibers - Hisian-fascicular tracts connect the atrium (atriofascicular pathways), AV node (nodofascicular pathways) or His bundle (fasciculoventricular) to distal Purkinje fibers or ventricular myocardium
Clinical manifestations
Wolff Parkinson White syndrome
- pre-excitation caused by accessory pathway - usually the Kent bundle, which directly links the atria to the ventricles, bypassing the atrioventricular (AV) node in combination with recurrent atrioventricular reentrant tachycardia
- The prevalence of WPW pattern is estimated at 0.13 to 0.25 % in the general population
- WPW can be divided by position of accessory pathway to:
- Type A - left sided accessory pathway resulting in tall R wave in leads V1-V3 (a positive or upward delta wave)
- Type B - right sided accessory pathway in which there are QS complexes in leads V1-V3 (a negative or downward delta wave)
The majority of patients with the WPW pattern on their ECG remain asymptomatic, although a small percentage of patients with the WPW pattern develop arrhythmias as a part of WPW syndrome.
The most frequent WPW associated tachycardia is AVRT.
Atrioventricular reentrant tachycardia (AVRT)
- AVRT is a supraventricular tachycardia that utilizes an accessory pathway between the atria and ventricles resulting in a circus movement.
- It is frequently, but not exclusively, associated with preexcitation syndrome (ie, the Wolff-Parkinson-White syndrome).
- The circuit involved in this reentrant arrhythmia includes the accessory bypass tract, AV node, and His Purkinje system, as well as the atria and ventricles.
- There is always 1:1 conduction of the impulse between the atria and ventricles since both structures, along with the AV node and accessory pathway, are a necessary part of the circuit.
- AVRT is often triggered by premature atrial beats or premature ventricular beats – retrograde activation of atria.
- Orthodromic AVRT accounts for >90% of AVRT and 20-30% of all sustained SVT.
Orthodromic AVRT
- >90% of AVRT
- re-entrant impulse goes from the atrium to the ventricle through the AV node (normal ventricular activation) and then retrogradely activates atria through accessory pathway
- ECG:
- narrow complex tachycardia
- ventricular rate 150-250 bpm
- inverted P wave following a QRS complex - retrograde activation of the atrium
- short RP interval that is usually less than half of RR interval (< ½ RR)
Antidromic AVRT
- the least common arrhythmia associated with WPW syndrome (3-8% of patients)
- Ventricles are activated through a very fast-conducting accessory pathway – anterograde conduction, atria are retrogradely activated over the AV node or another accessory pathway (30-60% of patients have multiple accessory pathways).
- ECG:
- wide QRS complex tachycardia
- ventricular rate 150-250 bpm
- Inverted P waves are often hidden in ST-T segment and therefore the RP interval is usually difficult to assess
Picture 1 Visualization of accessory pathway (bundle of Kent)
http://ems12lead.com/2012/02/06/discussion-for-17-year-old-male-cc-chest-pain-and-palpitations-wpw-part-i/#gref
Lown- Ganong-Levine syndrome
- short PR interval
- The exact mechanism of LGL has not been completely described. It’s most likely due to rapidly conducting fibers within the AV node
- Conduction occurs more rapidly than normal from the atria to the ventricles, explaining the short PR. The QRS complex is normal in duration and morphology since ventricular activation is via the normal conduction pathway.
Accessory pathway as a bystander
- In the presence of focal AT, atrial flutter, AF, or AVNRT
- QRS complexes can be pre-excited with delta waves when the AP acts as a bystander, and is not a critical part of the re-entry circuit.
FBI = Fast Broad Irregular tachycardia
- this arrhythmia represents a pre-excited atrial fibrillation
- Paroxysmal AF has been found in 50% of patients with WPW
- Typically young patients with no structural disease of the heart
- atrial fibrillation with fast ventricular response over an accessory pathway
- potentially life-threatening arrhythmia – due to 1:1 conduction the ventricular rate may be very rapid (even >300bpm) and it can degenerate into ventricular fibrillation!
ECG of atrial fibrillation in WPW:
- irregular wide complex tachycardia
- ventricular rate >200 bpm
- QRS complexes usually have variable morphology – APs bypassing the AV node can produce wide and bizarre looking complexes
- axis remains stable
Permanent junctional reciprocating tachycardia (PJRT)
- PJRT is a rare form of AV reciprocating tachycardia using a concealed AP
- Accessory pathways are usually located in the posteroseptal region and are associated with retrograde conduction
- PJRT is a long RP tachycardia due to slow conduction properties of the AP
- characterized by deeply inverted retrograde P waves in leads II, III, and aVF
- The incessant nature of PJRT may result in tachycardiomyopathy (TCM) that usually resolves after successful treatment by radiofrequency catheter ablation
ECG features of preexcitation
- preexcitation has a typical pattern during sinus rhythm:
- the PR interval is short
- delta wave - the initial part of ventricular activation is slowed, and the upstroke of the QRS complex is slurred, because of slow muscle-fiber-to-muscle-fiber conduction.
- wide QRS complex >120ms - the QRS complex represents a fusion beat - the initial part results from slow ventricular activation via the accessory pathway, while the terminal portion of ventricular activation is via the normal conduction system.
- ST segment and T wave abnormalities - reflecting abnormal ventricular repolarization.
- ST-T segment is usually directed opposite to delta waves > positive delta wave is often followed with a descending ST segment and inverted T wave.
- The more rapid the conduction along the accessory pathway, the greater the amount of myocardium depolarized via the accessory pathway > resulting in a more prominent or wider delta wave, and increasing prolongation of the QRS complex.
Delta waves can be misinterpreted as a different diagnosis due to similar patterns as:
- Myocardial infarction (MI) – A negative delta wave presented as a Q wave. On the other hand, a positive delta wave may mask the presence of a previous MI
- Ventricular premature beats (VPBs) or idioventricular rhythm – Intermittent WPW may be mistaken for frequent VPBs.
- Bundle branch block – The QRS duration is equal to or greater than 0.12 seconds because of preexcitation (the delta wave). Right-sided pre-excitation can be mistaken for LBBB; left sided pre-excitation can be mistaken for RBBB
Various algorithms have been developed to help determine pathway location from surface ECG. One of those is for example St. George’s algorithm:
Picture 2
BRUGADA and col. 2019 Guidelines on Supraventricular Tachycardia (for the management of patients with) [online]. [cit. 4.2.2021]. Accessible at WWW: https://academic.oup.com/eurheartj/article/41/5/655/5556821
ECG 1
Delta waves during sinus rhythm
- sinus rhythm at a rate of 60 bpm
- PR interval is shorter around 120ms
- typical sloping delta waves in every lead
- QRS complex is wide >120ms
- using St. George’s algorithm, we can approximate localization of the accessory pathway
- negative QRS complexes in leads V1 and III
- and negative QRS in lead aVF
- from there we can see highest R in lead V4 and R
- in conclusion the accessory pathway is probably located in mid septal region
ECG 2
Sinus rhythm with delta waves
- sinus rhythm at a rate of 57 bpm
- short PR interval – 90ms
- delta waves present
- wide QRS complexes – 150ms
- ST segment and T waves abnormalities – in leads II, III, aVF descending ST depression and inverted T wave with preceding positive delta wave
- location of accessory pathway by St. George’s algorithm – Right lateral location
- negative QRS in V1, positive QRS in III, positive QRS in aVL
Management
- risk stratification of asymptomatic patients with WPW pattern on a surface ECG using non-invasive tests (exercise ECG) or an electrophysiologic study
- Recommended long-term treatment for symptomatic patients is catheter ablation of the accessory pathway. Precise localization of the anomalous pathway is critical for successful ablation
- Symptomatic patients with tachyarrhythmias should be treated accordingly for the specific type of pre-excited arrhythmia.
References
- CAMM, A. J., LÜSCHER, T. F., & SERRUYS, P. W. (2009). The ESC textbook of cardiovascular medicine. Oxford, Oxford University Press
- Brugada J, Katritsis DG, Arbelo E, Arribas F, Bax JJ, Blomström-Lundqvist C, Calkins H, Corrado D, Deftereos SG, Diller GP, Gomez-Doblas JJ, Gorenek B, Grace A, Ho SY, Kaski JC, Kuck KH, Lambiase PD, Sacher F, Sarquella-Brugada G, Suwalski P, Zaza A; ESC Scientific Document Group. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur Heart J. 2020 Feb 1;41(5):655-720. doi: 10.1093/eurheartj/ehz467. PMID: 31504425.
- Jordan M Prutkin, MD, MHS, FHRS (2019). ECG tutorial: Preexcitation syndromes. In I. Gordon M Saperia, MD (Ed.), UpToDate. Retrieved February 3, 2021, from https://www-uptodate-com.ezproxy.is.cuni.cz/contents/ecg-tutorial-preexcitation-syndromes?search=preexcitation%20syndrome&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2
- Bradley P Knight, MD, FACC (2019). Anatomy, pathophysiology, and localization of accessory pathways in the preexcitation syndrome. In I. Todd F Dardas, MD, MS (Ed.), UpToDate. Retrieved February 3, 2021 from https://www-uptodate-com.ezproxy.is.cuni.cz/contents/anatomy-pathophysiology-and-localization-of-accessory-pathways-in-the-preexcitation-syndrome?search=preexcitation%20syndrome&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1
- Luigi Di Biase, MD, PhD, FHRS, Edward P Walsh, MD (2019). Wolff-Parkinson-White syndrome: Anatomy, epidemiology, clinical manifestations, and diagnosis. In I. Todd F Dardas, MD, MS (Ed.), UpToDate. Retrieved February 3, 2021 from https://www-uptodate-com.ezproxy.is.cuni.cz/contents/wolff-parkinson-white-syndrome-anatomy-epidemiology-clinical-manifestations-and-diagnosis?search=preexcitation%20syndrome&source=search_result&selectedTitle=3~150&usage_type=default&display_rank=3
Pictures
- BAUMRIND, David. EMS 12-Lead [online]. [cit. 3.2.2021]. Accessible at WWW: http://ems12lead.com/2012/02/06/discussion-for-17-year-old-male-cc-chest-pain-and-palpitations-wpw-part-i/#gref
- BRUGADA and col. 2019 Guidelines on Supraventricular Tachycardia (for the management of patients with) [online]. [cit. 4.2.2021]. Accessible at WWW: https://academic.oup.com/eurheartj/article/41/5/655/5556821




