
Introduction
Also known as "J-waves" or "J-point elevation. Early repolarization (ER) is characterized by J-point elevation of ≥0.1 mV in two adjacent leads with either a slurred or notched morphology.
The presence of an early repolarization pattern in the inferior and/or lateral leads has been associated with idiopathic VF in case–control studies.
ECG features
An elevated take-off of the ST segment at the J point of the QRS complex, varying from 1 to 4 mm relatively to isoelectric line.
- notch (J wave) or slur of QRS terminal portion
- upward concavity of ST segment
- positive concordant T waves
Classification
- Type 1 is associated with ER in the lateral precordial leads. This form is common among healthy male athletes and is thought to be largely benign
- Type 2 is associated with ER in the inferior or inferolateral leads and is associated with a moderate level of risk.
- Type 3 is associated with ER globally in the inferior, lateral, and right precordial leads, and appears to be associated with the highest relative risk, though the absolute risk of sudden death remains small
- Type 4, or Brugada syndrome, is marked by J-wave/point elevation in the right precordial leads.
Clinical manifestation
- ER pattern - describes the patient with appropriate ECG findings in the absence of symptomatic arrhythmias.
- ER syndrome - applies to the patient with both appropriate ECG findings and symptomatic arrhythmias.
Risk stratification
- Clinical features
- Family history of SCD
- J- wave amplitude
- J wave distribution
- J wave morfology
- ST segment (horizontal/descending)
Treatment
- ER pattern - nearly always a benign incidental ECG fading (no specific signs or symptoms) – AHA and ESC do not recommend any specific treatment
- ER syndrome with VF - ICD implantation
- for patients with recurrent VF - quinidine
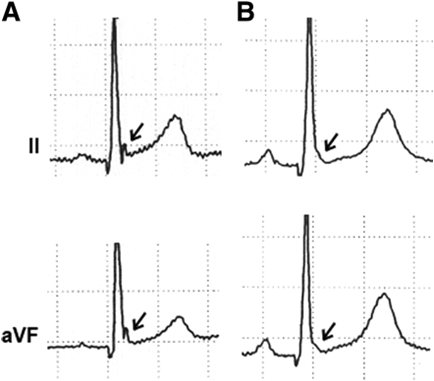
ECG 1 Patient with in hospital cardiac arrest due to VF (signs of ER in inferolateral leads)

References
- Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, Kirchhof P, Kjeldsen K, Kuck KH, Hernandez-Madrid A, Nikolaou N, Norekvål TM, Spaulding C, Van Veldhuisen DJ; Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC)Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Europace. 2015 Nov;17(11):1601-87. doi: 10.1093/europace/euv319. Epub 2015 Aug 29. PMID: 26318695.
- Haïssaguerre M, Derval N, Sacher F, et al. Sudden cardiac arrest associated with early repolarization. N Engl J Med. 2008 May 8;358(19):2016-23.
- Tikkanen JT, Anttonen O, Junttila MJ, Aro AL, Kerola T, Rissanen HA, Reunanen A, Huikuri HV. Long-term outcome associated with early repolarization on electrocardiography. N Engl J Med. 2009 Dec 24;361(26):2529-37. doi: 10.1056/NEJMoa0907589. Epub 2009 Nov 16. PMID: 19917913.
- https://www.uptodate.com/contents/early-repolarization

Introduction
Also known as "J-waves" or "J-point elevation. Early repolarization (ER) is characterized by J-point elevation of ≥0.1 mV in two adjacent leads with either a slurred or notched morphology.
The presence of an early repolarization pattern in the inferior and/or lateral leads has been associated with idiopathic VF in case–control studies.
ECG features
An elevated take-off of the ST segment at the J point of the QRS complex, varying from 1 to 4 mm relatively to isoelectric line.
- notch (J wave) or slur of QRS terminal portion
- upward concavity of ST segment
- positive concordant T waves
Classification
- Type 1 is associated with ER in the lateral precordial leads. This form is common among healthy male athletes and is thought to be largely benign
- Type 2 is associated with ER in the inferior or inferolateral leads and is associated with a moderate level of risk.
- Type 3 is associated with ER globally in the inferior, lateral, and right precordial leads, and appears to be associated with the highest relative risk, though the absolute risk of sudden death remains small
- Type 4, or Brugada syndrome, is marked by J-wave/point elevation in the right precordial leads.
Clinical manifestation
- ER pattern - describes the patient with appropriate ECG findings in the absence of symptomatic arrhythmias.
- ER syndrome - applies to the patient with both appropriate ECG findings and symptomatic arrhythmias.
Risk stratification
- Clinical features
- Family history of SCD
- J- wave amplitude
- J wave distribution
- J wave morfology
- ST segment (horizontal/descending)
Treatment
- ER pattern - nearly always a benign incidental ECG fading (no specific signs or symptoms) – AHA and ESC do not recommend any specific treatment
- ER syndrome with VF - ICD implantation
- for patients with recurrent VF - quinidine
ECG 1 Patient with in hospital cardiac arrest due to VF (signs of ER in inferolateral leads)
References
- Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, Kirchhof P, Kjeldsen K, Kuck KH, Hernandez-Madrid A, Nikolaou N, Norekvål TM, Spaulding C, Van Veldhuisen DJ; Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC)Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Europace. 2015 Nov;17(11):1601-87. doi: 10.1093/europace/euv319. Epub 2015 Aug 29. PMID: 26318695.
- Haïssaguerre M, Derval N, Sacher F, et al. Sudden cardiac arrest associated with early repolarization. N Engl J Med. 2008 May 8;358(19):2016-23.
- Tikkanen JT, Anttonen O, Junttila MJ, Aro AL, Kerola T, Rissanen HA, Reunanen A, Huikuri HV. Long-term outcome associated with early repolarization on electrocardiography. N Engl J Med. 2009 Dec 24;361(26):2529-37. doi: 10.1056/NEJMoa0907589. Epub 2009 Nov 16. PMID: 19917913.
- https://www.uptodate.com/contents/early-repolarization




