
Introduction
Takotsubo cardiomyopathy (TTC), also called stress‐induced cardiomyopathy, broken heart syndrome or apical ballooning cardiomyopathy was first described in 1990 in Japan.
It is characterized by a transient, reversible, regional systolic and diastolic dysfunction usually involving the left ventricular apex and mid ventricle with hyperkinesia of the basal left ventricular segments.
Why Takotsubo? The left ventricle, with its apical akinesia and ballooning looks remarkably like a pot used by Japan fisherman to trap octopuses.

https://www.ahajournals.org/doi/full/10.1161/CIRCULATIONAHA.108.767012
It occurs predominantly in women, especially after menopause. Most people recover with no long-term heart damage.
The early clinical presentation is very similar to acute coronary syndrome (ACS), but on angiography patients have normal coronary arteries. The main symptoms are chest pain and shortness of breath.
Etiology
Contemporary, the most accepted theory is myocardial stunning caused by high concentrations of circulating catecholamines.
Catecholamines are directly toxic to the myocardium and secondarily cause transient microvascular dysfunction.
It is not clear why some people develop the disease after being exposed to the provoking factors and others do not.
The genetic predisposition to the effect of catecholamines and other substances on the myocardium probably plays a role.
ECG manifestation
- ST elevations
- T inversion
- No reciprocal ST depressions
- absence of Q waves
- QT interval prolongation
How to differentiate between STEMI ?
- ST elevations in TTC are most commonly in precordial leads
- ST elevations in TTC are usually not present in V1, in contrast ST elevations are usually present in aVR

Kosuge M, Ebina T, Hibi K, Morita S, Okuda J, Iwahashi N. Simple and accurate electrocardiographic criteria to differentiate takotsubo cardiomyopathy from anterior acute myocardial infarction. J Am Coll Cardiol. 2010;55(22):2514–6. doi: 10.1016/j.jacc.2009.12.059
ECG 1 Electrocardiogram demonstrating 1 mm ST segment elevations in V2-V3, I, aVL, +- aVR in a patient with Takotsubo cardiomyopathy caused by excessive emotional stress

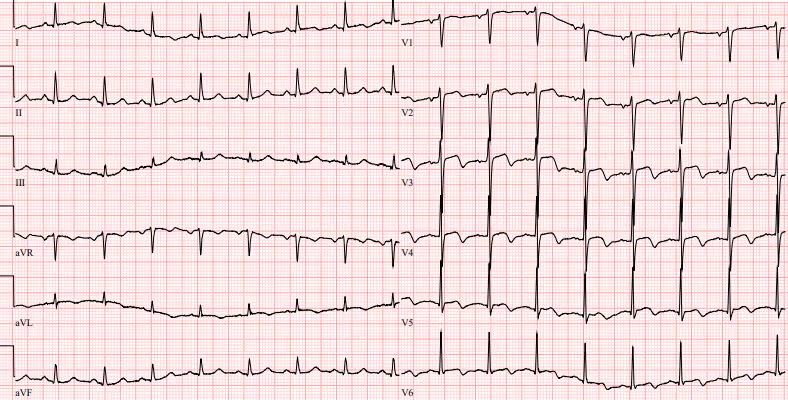
ECG 2 Electrocardiogram demonstrating ST segment elevations in V2-V3, I. Biphasic negative T waves V2-V6. Also note the slightly prolonged QTc interval.
Management
- coronary angiography to exclude acute myocardial infarction
- beta blockers
- ACE inhibitors
- anxiolytics
- diuretics
References
- Namgung J. Electrocardiographic Findings in Takotsubo Cardiomyopathy: ECG Evolution and Its Difference from the ECG of Acute Coronary Syndrome. Clin Med Insights Cardiol. 2014;8:29-34. Published 2014 Mar 13. doi:10.4137/CMC.S14086
- Takotsubo cardiomyopathy (broken-heart syndrome) - Harvard Health. Health Information and Medical Information - Harvard Health [online]. Copyright © 2010 [cit. 04.02.2021]. Dostupné z: https://www.health.harvard.edu/heart-health/takotsubo-cardiomyopathy-broken-heart-syndrome
- MANN, Douglas L, et al. Braunwald´s Heart Disease : A Textbook of Cardiovascular Medicine. 10th Edition. 2015. ISBN 978-0-323-29429-4.
- MEDINA DE CHAZAL, Horacio, Marco Giuseppe DEL BUONO a Lori KEYSER-MARCUS. Stress Cardiomyopathy Diagnosis and Treatment. Journal of the American College of Cardiology. 2018, vol. 72, s. 1955-1971, ISSN 0735-1097. DOI: 10.1016/j.jacc.2018.07.072.
- FRANGIEH, A. H., S. OBEID, J. R. GHADRI, et al. ECG Criteria to Differentiate Between Takotsubo (Stress) Cardiomyopathy and Myocardial Infarction. Journal of the American Heart Association [online]. 2016, 5(6) [cit. 2021-02-04]. ISSN 20479980. Dostupné z: doi:10.1161/JAHA.116.003418
- Kosuge M, Ebina T, Hibi K, Morita S, Okuda J, Iwahashi N. Simple and accurate electrocardiographic criteria to differentiate takotsubo cardiomyopathy from anterior acute myocardial infarction. J Am Coll Cardiol. 2010;55(22):2514–6. doi: 10.1016/j.jacc.2009.12.059
.jpg)
Introduction
Takotsubo cardiomyopathy (TTC), also called stress‐induced cardiomyopathy, broken heart syndrome or apical ballooning cardiomyopathy was first described in 1990 in Japan.
It is characterized by a transient, reversible, regional systolic and diastolic dysfunction usually involving the left ventricular apex and mid ventricle with hyperkinesia of the basal left ventricular segments.
Why Takotsubo? The left ventricle, with its apical akinesia and ballooning looks remarkably like a pot used by Japan fisherman to trap octopuses.
https://www.ahajournals.org/doi/full/10.1161/CIRCULATIONAHA.108.767012
It occurs predominantly in women, especially after menopause. Most people recover with no long-term heart damage.
The early clinical presentation is very similar to acute coronary syndrome (ACS), but on angiography patients have normal coronary arteries. The main symptoms are chest pain and shortness of breath.
Etiology
Contemporary, the most accepted theory is myocardial stunning caused by high concentrations of circulating catecholamines.
Catecholamines are directly toxic to the myocardium and secondarily cause transient microvascular dysfunction.
It is not clear why some people develop the disease after being exposed to the provoking factors and others do not.
The genetic predisposition to the effect of catecholamines and other substances on the myocardium probably plays a role.
ECG manifestation
- ST elevations
- T inversion
- No reciprocal ST depressions
- absence of Q waves
- QT interval prolongation
How to differentiate between STEMI ?
- ST elevations in TTC are most commonly in precordial leads
- ST elevations in TTC are usually not present in V1, in contrast ST elevations are usually present in aVR
Kosuge M, Ebina T, Hibi K, Morita S, Okuda J, Iwahashi N. Simple and accurate electrocardiographic criteria to differentiate takotsubo cardiomyopathy from anterior acute myocardial infarction. J Am Coll Cardiol. 2010;55(22):2514–6. doi: 10.1016/j.jacc.2009.12.059
ECG 1 Electrocardiogram demonstrating 1 mm ST segment elevations in V2-V3, I, aVL, +- aVR in a patient with Takotsubo cardiomyopathy caused by excessive emotional stress
ECG 2 Electrocardiogram demonstrating ST segment elevations in V2-V3, I. Biphasic negative T waves V2-V6. Also note the slightly prolonged QTc interval.
Management
- coronary angiography to exclude acute myocardial infarction
- beta blockers
- ACE inhibitors
- anxiolytics
- diuretics
References
- Namgung J. Electrocardiographic Findings in Takotsubo Cardiomyopathy: ECG Evolution and Its Difference from the ECG of Acute Coronary Syndrome. Clin Med Insights Cardiol. 2014;8:29-34. Published 2014 Mar 13. doi:10.4137/CMC.S14086
- Takotsubo cardiomyopathy (broken-heart syndrome) - Harvard Health. Health Information and Medical Information - Harvard Health [online]. Copyright © 2010 [cit. 04.02.2021]. Dostupné z: https://www.health.harvard.edu/heart-health/takotsubo-cardiomyopathy-broken-heart-syndrome
- MANN, Douglas L, et al. Braunwald´s Heart Disease : A Textbook of Cardiovascular Medicine. 10th Edition. 2015. ISBN 978-0-323-29429-4.
- MEDINA DE CHAZAL, Horacio, Marco Giuseppe DEL BUONO a Lori KEYSER-MARCUS. Stress Cardiomyopathy Diagnosis and Treatment. Journal of the American College of Cardiology. 2018, vol. 72, s. 1955-1971, ISSN 0735-1097. DOI: 10.1016/j.jacc.2018.07.072.
- FRANGIEH, A. H., S. OBEID, J. R. GHADRI, et al. ECG Criteria to Differentiate Between Takotsubo (Stress) Cardiomyopathy and Myocardial Infarction. Journal of the American Heart Association [online]. 2016, 5(6) [cit. 2021-02-04]. ISSN 20479980. Dostupné z: doi:10.1161/JAHA.116.003418
- Kosuge M, Ebina T, Hibi K, Morita S, Okuda J, Iwahashi N. Simple and accurate electrocardiographic criteria to differentiate takotsubo cardiomyopathy from anterior acute myocardial infarction. J Am Coll Cardiol. 2010;55(22):2514–6. doi: 10.1016/j.jacc.2009.12.059


